Coronavirus Technology Solutions
July 14, 2020
Healthy Lifestyle Along with Coronavirus Technology and Pharmaceutical Solutions will Vanquish COVID-19
Staten Island Mall Equates MERV 13 with HEPA Filters
A MERV 13 May or May Not be Enough When All the Parameters are Considered
Experts Continue to Push WHO to Recognize the Threat of Airborne Transmission
Ascend Performance Materials has New Nanofiber Mask
______________________________________________________________________________
Healthy Lifestyle Along with Coronavirus Technology and Pharmaceutical Solutions will Vanquish COVID-19
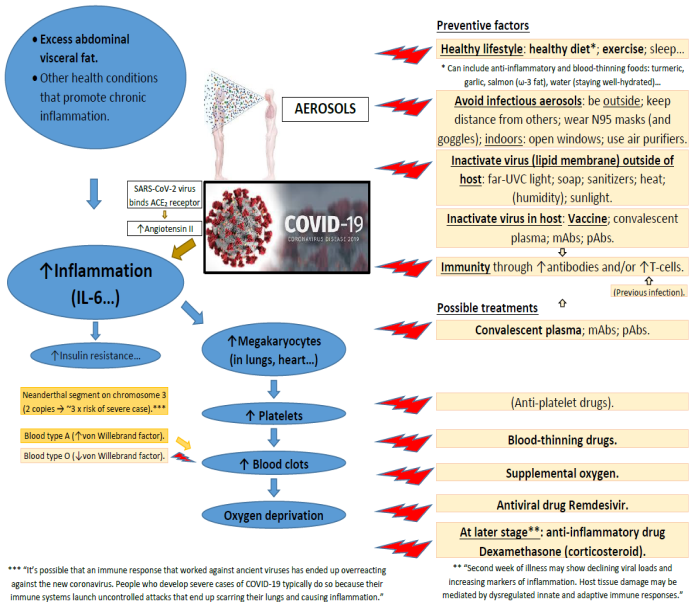
With a combination of Technology and Pharmaceutical Solutions COVID can be vanquished and near normal life quickly restored. McIlvaine has programs in both these areas but realizes there is a third weapon which is of equal importance - a healthy lifestyle. The recent wave of infections has resulted in younger people being hospitalized. Their recovery to full health will be affected by their health at the time of admission. Dr. Amy Anderson is a nutritional epidemiologist who focuses on how diet and other lifestyle behaviors can influence health. Amy has prepared the following diagram to show the interaction of a healthy lifestyle with the technology and pharmaceutical solutions.
Click here for a larger display
A healthy diet, exercise, and other healthy lifestyle behaviors could lower the risk of severe COVID-19 in part through their anti-inflammatory effects. For example, a healthy diet and overall lifestyle can help prevent or reduce excess abdominal visceral fat, which is a strong predictor of chronic, low-level inflammation (as measured by inflammatory cytokines such as interleukin-6 (IL-6)). Underlying chronic inflammation could exacerbate the inflammatory effects of SARS-CoV-2 viral infection and lead to more severe COVID-19. It thus appears optimal to try to reduce underlying inflammation through a healthy diet and overall lifestyle.
Dr. Amy Anderson can be reached at e-mail amylouiseanderson@yahoo.com.
Sources:
Coronavirus autopsies: A story of 38 brains, 87 lungs and 42 hearts. https://www.washingtonpost.com/health/2020/07/01/coronavirus-autopsies-findings/
Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. https://www.nejm.org/doi/full/10.1056/NEJMoa2021680?query=featured_home
DNA Inherited From Neanderthals May Increase Risk of Covid-19. https://www.nytimes.com/2020/07/04/health/coronavirus-neanderthals.html
Complications from COVID-19 may depend on von Willebrand factor in the blood. https://medicalxpress.com/news/2020-07-complications-covid-von-willebrand-factor.html
The McIlvaine Company provides Coronavirus Technology Solutions and Coronavirus Pharmaceutical Solutions. Information on these programs is found at www.mcilvainecompany.com
Bob McIlvaine can answer your questions at rmcilviane@mcilvainecompany.com; cell 847 226 2391
Staten Island Mall Equates MERV 13 with HEPA Filters
The Staten Island Mall has equipped its air conditioning system with new filters that will allow the New Springville shopping center to open in Phase 4 and protect consumers against the coronavirus (COVID-19). However, it is attributing more capability to MERV 13 filters than is warranted. MERV 13 filters are not HEPA filters and are likely to remove less than 75 percent of the virus particles.
The mall promoters say that even before Gov. Andrew Cuomo announced that malls would need enhanced air filtration systems in place to reopen, Staten Island Mall management had invested in more than 100 high-powered air filters, known as MERV-13 filters. This was according to James Easley, mall senior manager.
Filtration is a major function. It can filter out the COVID virus ... You have to have a MERV-13 for a large congregate setting. That would be the best,” said Cuomo on Monday at his press conference according to the mall announcement but that is not what we reported.
Easley said the Mall had conducted extensive research and found the MERV-13 to be the best filter to use in the common areas of the shopping center.
“The MERV-13 filter is similar to a HEPA filter. It catches 95 percent of all particulate materials from the air. Apparently, that’s enough to catch the virus,” said Easley. “Every one of our common areas have had these filters installed within the last week.”
Many websites tout the MERV-13 as the most effective filter according to Easley
“The MERV 13 (A.K.A. the Best filter) is our top model. It is electrostatically charged and constructed of materials that are more efficient than your standard poly-cotton pleated filters or fiberglass filters,” advertises Qualityairfilters.com.
“In fact, it is so effective it can filter out particles that are smaller than one micron in size. It is not chemically treated, so it promotes a healthy breathing environment, and it will not allow the growth of bacteria, mold, mildew, or fungi as long as it is used how it was meant to be used,” says the ad. So this was how it was reported by the Mall
A MERV 13 May or May Not be Enough When All the Parameters are Considered
We have covered MERV ratings in many articles easily found through a MERV search on the home page Here is how we covered the Cuomo guidance.
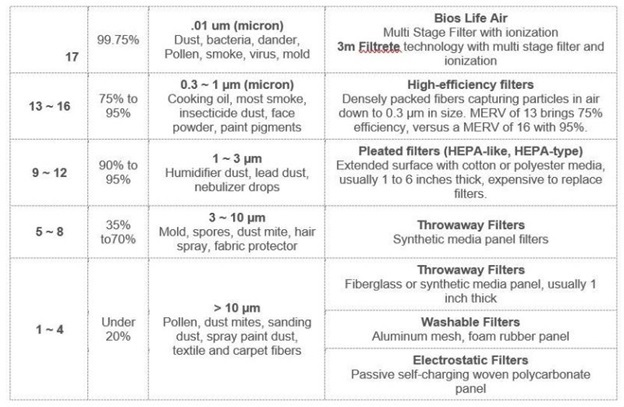
In his edict to New York mall owners, Cuomo was talking about HEPA filters, which have the highest MERV ratings, between 17 and 20.
What's MERV? It stands for "minimum efficiency reporting value," and it's how filters are rated in their ability to trap tiny particles. The MERV ratings go from one to 20. Filters with higher MERV ratings are more effective than filters with lower ratings.
At the highest end, HEPA filters are used by hospitals to create sterile rooms for surgeries and to control infectious diseases, and are able to remove 99.97 percent of dust, pollen, mold, bacteria and other airborne particles with a size as small as 0.3 microns. For comparison, Covid-19 is thought to be between 0.06 to 1.4 microns.
"Filters are rated at their worst performance, so 99.97 percent is the worst it will do," Allen said. "And that's rated for a particle size of 0.3 microns, but smaller and larger it actually does better. So the point is that it's capturing nearly all particles."
Unfortunately, most businesses and home owners may find it difficult to retrofit their existing system to accommodate a HEPA filter, or any filter higher than the rating recommended by the system's manufacturer.
Doing so can actually impair the system's performance. Smaller pores in HEPA air filters make it more difficult for it to push air. Using denser filters can affect the efficiency of the unit and strain the fan, while decreasing indoor air quality -- the opposite of what you desire.
"HEPA filtration is not always going to be feasible or practical," Allen said. "But there are other filters that can do the job. What is recommended now by the standard setting body for HVAC is a MERV 13 filter."
High-efficiency filters in the 13-to-16 MERV range are often used in hospitals, nursing homes, research labs and other places where filtration is important.
In our March 30 Alert we furnished the following comparison. Keep in mind that HEPA filters are MERV 17-20. MERV 13 filters would at best remove 75 percent of the virus particles.
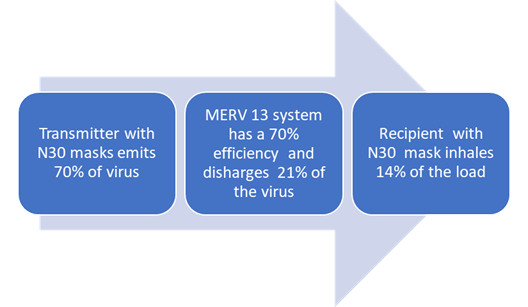
MERV 13 filters removing 75 percent of the virus are a big improvement over less efficient filters. Their effectiveness is as much affected by the volume and direction. The number of air changes per hour and the quantity of air which flows from a transmitter into the HVAC system as opposed to from transmitter to recipient and then the air filter system is important. This in turn is a function of the number of shoppers and the mask efficiency of each of the transmitters. If they are wearing N30 masks the efficiency is only 70 percent.
In the case of optimal air flow the transmitter with his N30 mask is only emitting 70 percent of the potential virus. If this goes directly into a MERV 13 system the recipient would at most be experience 21 percent of the viral load. If he is wearing an N30 mask he would inhale 14 percent of the load.
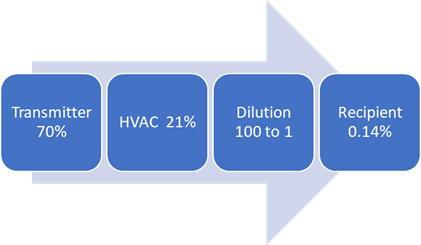
This hypothetical example assumes that all the virus from the transmitter is treated in the HVAC system and then all flows to the recipient. In fact there will be considerable dilution. But even if the dilution is 100 to one the recipient could be inhaling 0.14 percent of the load. If the transmitter is emitting thousands of particles per minute the recipient could be inhaling 14 virus particles per minute. Ten virus particles is said to be the minimum load necessary to cause infection.
A single breath releases 50 - 5000 droplets. Most of these droplets are low velocity and fall to the ground quickly. There are even fewer droplets released through nose-breathing. Importantly, due to the lack of exhalation force with a breath, viral particles from the lower respiratory areas are not expelled. If a person is infected, the droplets in a single cough or sneeze may contain as many as 200,000,000 (two hundred million) virus particles which can all be dispersed into the environment around them.
If a person coughs or sneezes, those 200,000,000 viral particles go everywhere. Some virus hangs in the air, some falls onto surfaces, most falls to the ground. So if you are face-to-face with a person, having a conversation, and that person sneezes or coughs straight at you, it's pretty easy to see how it is possible to inhale 1,000 virus particles and become infected.
But even if that cough or sneeze was not directed at you, some infected droplets - the smallest of the small - can hang in the air for a few minutes, filling every corner of a modest sized room with infectious viral particles. All you have to do is enter that room within a few minutes of the cough/sneeze and take a few breaths and you have potentially received enough virus to establish an infection.
But with general breathing, 20 viral particles minute into the environment, even if every virus ended up in your lungs (which is very unlikely), you would need 1000 viral particles divided by 20 per minute = 50 minutes.
Speaking increases the release of respiratory droplets about 10 fold; ~200 virus particles per minute. Again, assuming every virus is inhaled, it would take ~5 minutes of speaking face-to-face to receive the required dose.
The exposure to virus x time formula is the basis of contact tracing. Anyone you spend greater than 10 minutes with in a face-to-face situation is potentially infected. Anyone who shares a space with you (say an office) for an extended period is potentially infected.
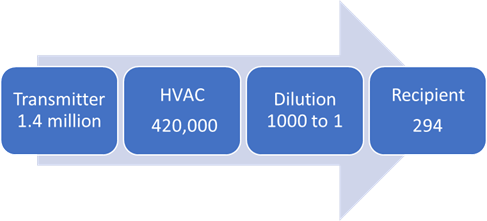
Assume in the mall situation that the transmitter generates 2 million viral particles. His mask will reduce the transmission to 1.4 million particles. The HVAC system will reduce the load to 420,000 and then dilute it 1000 times. The recipient wearing an N30 mask will reduce the 420 particles to 294. This could be a one time event or it could happen every minute or two while both transmitter and recipient are in the area covered by the HVAC system.
The variables are huge. There can be multiple transmitters in the range of one HVAC system. Their virus particle generation will be uneven. The amount of dilution is another variable. However there are sufficient numbers of viral particles being generated by just one super spreader that the higher the efficiency of removal at each stage the better.
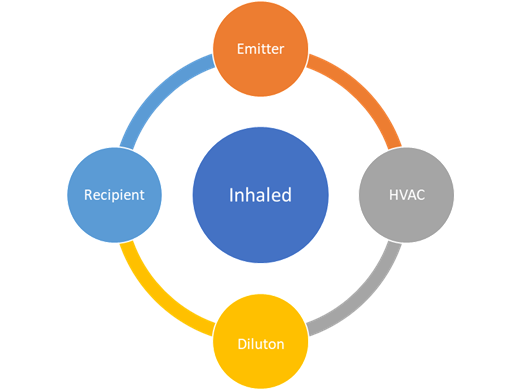
The minimization of inhalation depends on a clockwise sequence which includes the HVAC and dilution prior to the virus reaching the recipient. In the counter clockwise sequence the virus cloud moves from the emitter directly to the recipient.
|
Mask Type |
Emitter |
HVAC |
Dilution |
Recipient |
|
N30 masks |
1,400,000 |
x |
x |
980,000 |
|
N95 masks |
100,000 |
x |
x |
5000 |
|
N99 Masks |
20,000 |
x |
x |
200 |
|
N100 Masks |
2000 |
x |
x |
2 |
If transmitter and recipient are wearing N30 masks the recipient inhales almost 1 million particles. If they were both to wear N99 masks the recipient inhales only 200 particles. So N99 masks even without HVAC and dilution are just as safe as N30 masks with 70% efficient HVAC and 1000 to 1 dilution.
Mall owners should examine these statistics carefully. They may want to consider renting N100 powered respirators to shoppers.
Experts Continue to Push WHO to Recognize the Threat of Airborne Transmission
The World Health Organization (WHO) is preparing a scientific brief to address the continually emerging evidence on transmission of COVID-19 and plans to release its guidance "in the coming days."
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
"Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control," lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
"This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die," said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. "We wanted to bring this to the attention of the world to prevent this from happening."
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
"We have been working on a scientific brief…to consolidate knowledge around transmission," she added.
One focus will be on how masks protect healthcare workers. "We are also looking at the possible role of airborne transmission in other settings." Van Kerkhove said. "We will be releasing our brief in the coming days."
"We acknowledge there is emerging evidence in this field," Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. "Therefore, we believe we have to be open to this evidence and its implications."
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. "Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance," she said. Another aim was determining the dose of the virus required for airborne transmission.
"These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated," she explained.
In the meantime, Allegranzi said, "the possibility of airborne transmission in public settings — especially closed, poorly ventilated settings — cannot be ruled out."
Morawska said the evidence already exists. "A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation." As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for "national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation."
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need "to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. "Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible," she said during the press briefing. "We have to consider the weight of the evidence."
"We are constantly looking for information on how we can do better," Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a "living systematic review" — updating the consensus of evidence on a weekly basis.
"This process on COVID-19 will, I am sure, continue for the weeks and months to come," she added.
Ascend Performance Materials has New Nanofiber Mask
Ascend Performance Materials has developed a new mask technology that protect against SARS-CoV-2.
The masks, a nanofiber and a microfiber nonwoven version each branded under the Acteev Biodefend line for medical devices, deliver a one-two punch of antiviral properties plus top-level barrier protection against microbes, harmful airborne particles and fluid splatter, according to the company.
“The material that goes into this material is made in Pensacola. We’ve submitted a filing with the FDA to market technology in a surgical mask that lab tests show to be 99% effective against SARS-CoV-2,” Nicki Britton, Ascend’s global communications manager, told NorthEscambia.com. “It’s a new way of achieving efficacy – our scientists and engineers have invented a process for embedding active zinc ions into soft nylon, resulting in a fabric that is both antiviral and comfortable. The mask designs we filed also achieve top level filtration.”
“We’ve been working on this technology for several years. When the pandemic hit we shifted our business to answer this immediate need. Our products are manufactured in the U.S.A.,” Britton said.
Ascend has filed the necessary paperwork with the FDA to market the masks and is hoping for approval soon.
Acteev technology has been shown in laboratory tests to deactivate SARS-CoV-2, the coronavirus that causes COVID-19, and other pathogens including H1N1, betacoronavirus OC43, human coronavirus 229E and Gram-positive and Gram-negative bacteria such as staphylococcus and E. coli, according to Vikram Gopal, Ph.D., Ascend’s chief technology officer. The testing was conducted following the protocols of ISO, ASTM or other international standards organizations.
The proposed masks also meet the requirements to qualify as Level III standards, as tested by independent laboratories as well as Ascend scientists. Level III is the highest tier for physical barrier and safety properties, according to the common international testing standard.
Dr. Gopal said the combination of superior physical properties and antiviral protection is a breakthrough in medical device technology, as many masks succeed either at antiviral protection or at filtration and barrier effectiveness but not at both.
“Previous technologies rely on the materials within a mask to retain an electrical charge to achieve filtration efficiency,” Dr. Gopal said. “But when antimicrobial agents are added, those materials lose their charge and begin to fail as barriers.”
Acteev masks, however, achieve antiviral effectiveness through active zinc ions embedded within the polymer structure of polyamide 66, a hygroscopic nylon material whose equilibrium moisture keeps the zinc ions active.
“With Acteev, we have cracked the code of balancing top physical performance with antiviral protection,” Dr. Gopal said.
The technology, covered by more than 15 patent families, has been tested in multiple end forms, including knit and woven fabrics; engineered plastics; and nanofiber meltblown, microfiber meltblown and spunbond nonwoven materials.